 Actually, it’s more the change of location that’s made a difference. I’m finally back in the zone with the book. Writing like a demon…
Actually, it’s more the change of location that’s made a difference. I’m finally back in the zone with the book. Writing like a demon…
What a difference a day makes
Reply
Actually, it’s more the change of location that’s made a difference. I’m finally back in the zone with the book. Writing like a demon…
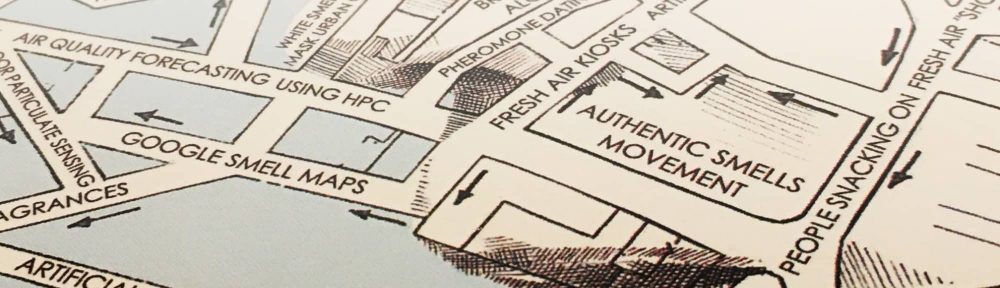
Leaked internal video from Google. Play video here.  .
.

There is something so wonderful about this. A way to attack hatred and fear with wit and playfulness. A see saw through the US border fence. More here.
Examples of how dreams have led to the creation of musical masterpieces are legion and include the story, related by neurologist Oliver Sacks, of Wagner literally dreaming up the introduction to Das Rheingold while in a semi-sleeping or somnolent state. Ravel, Mozart, Chopin, Brahms, and Stravinsky similarly stated that melodies came to them in dreams or daydreams.
The fact that music is abstract in nature is relevant to any dis- cussion about ideas. As Sacks said in his book Musicophelia, “the neural processes underlying that which we call creativity have nothing to do with rationality. That is to say, if we look at how the brain generates creativity, we will see that it is not a rational process at all; creativity is not born out of reasoning.” Philip Ball, author of The Music Instinct, says that music is “a remark- able blend of art and science, logic and emotion, physics and psychology.”
How can music influence the generation of new ideas? One possible explanation is that electrical discharges from neural networks might resemble music if they were communicated acoustically. This could explain how music somehow helps to highlight information or feelings that have otherwise been for- gotten, unnoticed, or repressed. In other words, music may influence thinking in a manner that is similar to dreaming. Dreaming and music can both bypass logic, and both can trigger thoughts deep inside the brain stem or connect visual images in the cortex. Incidentally, if you are wondering whether listening to music while doing something else counts as multitasking, the answer is no. According to Dr. Clifford Ness, a professor at Stanford University, the modality of instrumental music doesn’t appear to create any negative consequences.
Brain imaging techniques have demonstrated that while some professional musicians’ brains are shaped slightly differently from those of nonmusicians, musicality exists in virtually every- one. Moreover, while listening to Bach certainly won’t turn you into Mozart, exposure to classical music appears to enhance the mathematical and verbal skills of individuals at quite an early age.
Remember also the mnemonic power of music. Think back to your childhood or, if that’s too far away, perhaps your own children. Were you sung to, or did you sing songs, to remember complex ideas? Your instant reaction is possibly “No.” But perhaps you don’t think of music in this way. Surely you were taught the alphabet using a rhyme? A, B, C, D, E, F, G… H, I, J, K, LMNOP. Similar tricks are used with older students to help them memorize everything from periodic tables to US Presidents and the technique has been used across all kinds of cultures.
Music and language almost certainly have common origins and the use of music and pictures to convey information and ideas goes back to the earliest days. This is partly because it is easier for most people to remember information or ideas via association or stories than as facts alone.
It does strike me that music and stories are underutilized in the organizational context. Music in particular has the power to make people alert, but also to awaken deep thinking. Music can trigger feelings (something Nietzsche, a lifelong depressive, wrote of frequently), which in turn produce thoughts and images in our minds—it is these thoughts and images that can become novel solutions and innovative new ideas. Music is therefore directly related to the production of new ideas.
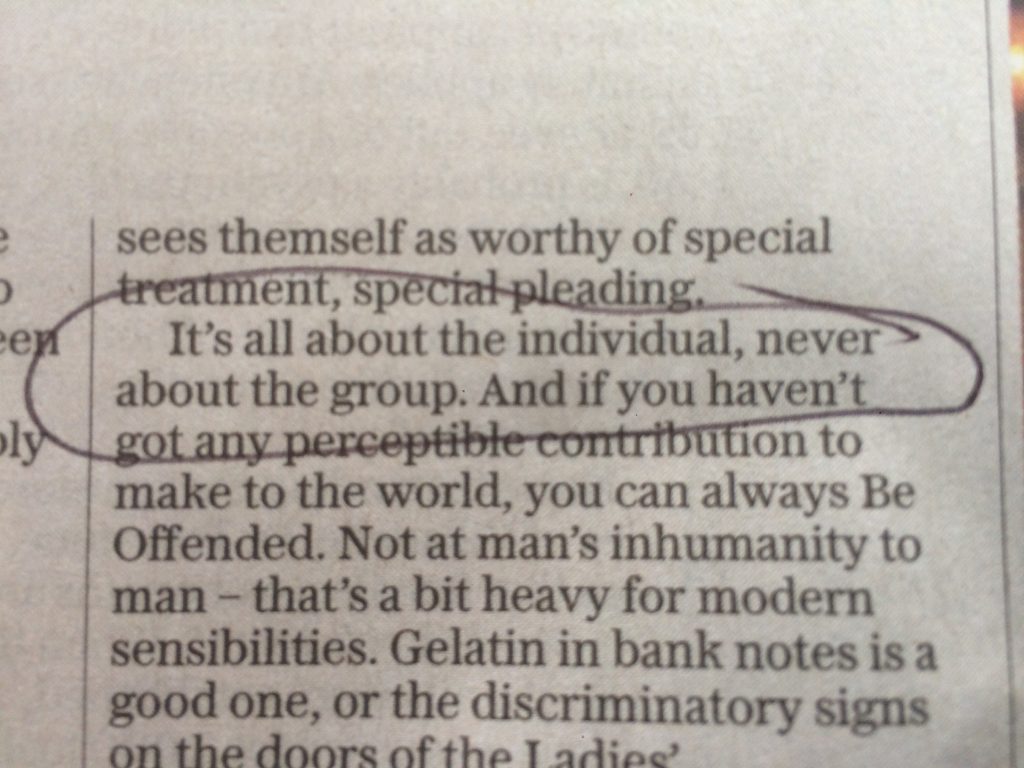
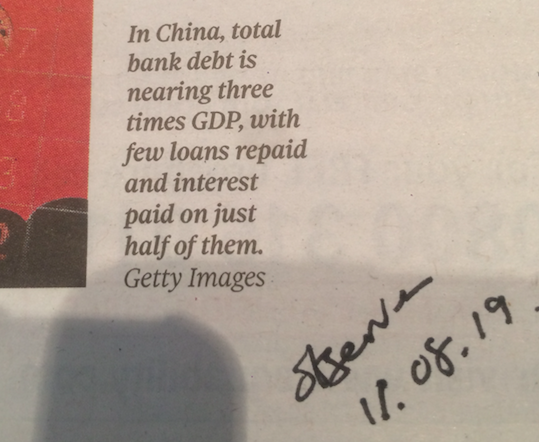
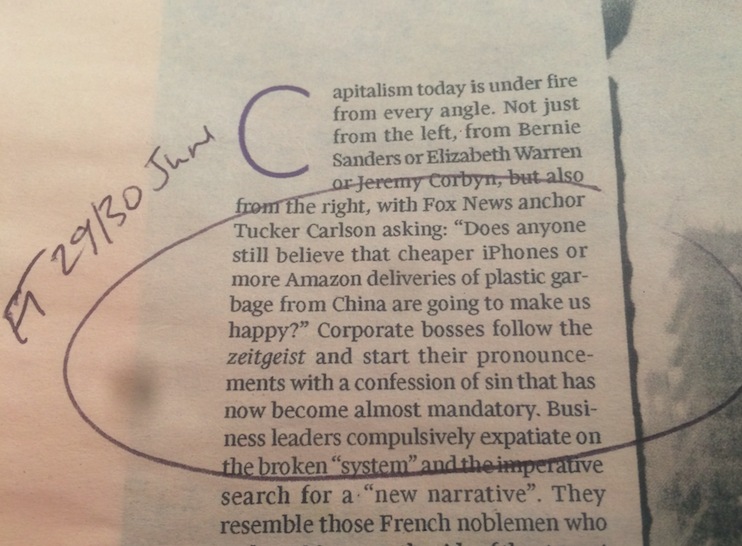
Can’t remember where I saw this – a newspaper. Bang on the money if you ask me. But could things swing back to the group? Could responsibilities triumph over rights?